
Skin barrier damage and acne can look annoyingly similar. Both can cause redness, rough texture, bumps, inflamed spots, and sudden breakouts. The difference is that they are not the same problem. Acne is a disorder of the pilosebaceous unit, meaning the hair follicle and oil gland. Barrier damage is a disruption of the stratum corneum, the outermost protective layer of the skin. You can have either one alone, or both at the same time.[1][11]
If your skin suddenly burns, stings, feels tight, flakes, and reacts to products that used to be fine, think damaged barrier first. If you have blackheads, whiteheads, recurring oily-zone breakouts, deep painful nodules, or cysts, acne is more likely. If you have acne plus burning, peeling, and sensitivity after starting actives, you probably have both.
The fastest clue is this: barrier damage usually feels wrong everywhere, while acne usually forms recognizable follicle-based lesions.
Damaged Skin Barrier: Signs and Repair | Why Does My Moisturizer Burn? | The Ordinary Glycolic Acid 7% Review | Best Moisturizers for Oily, Acne-Prone Skin
What is in this article
1. What the skin barrier actually is
The skin barrier mainly refers to the stratum corneum, the thin outer layer of the epidermis. Dermatology papers often describe it as a brick-and-mortar structure. The bricks are corneocytes, which are flattened, protein-rich, terminally differentiated cells. The mortar is a lipid matrix made mainly of ceramides, cholesterol, and free fatty acids arranged in lamellar sheets. This structure keeps water in and helps keep irritants, allergens, pollutants, and microbes out.[1][3][4]
A healthy barrier is not just a passive wall. It helps regulate hydration, desquamation, surface pH, antimicrobial defense, immune signaling, and the skin microbiome. When it is intact, the skin is better at tolerating normal skincare and environmental stress. When it is disrupted, the same routine can suddenly feel like it is attacking your face.[1][7]
The lipid matrix matters
The intercellular lipid matrix is central to barrier function. A useful shorthand is that stratum corneum lipids are dominated by ceramides, cholesterol, and free fatty acids. Exact proportions vary by body site, age, disease state, and measurement method, so it is better to say these lipids work as a coordinated system rather than claiming one universal perfect ratio for every face.[1][4][9]
TEWL: the barrier measurement people talk about
Transepidermal water loss, usually shortened to TEWL, measures the passive movement of water vapor from inside the body through the epidermis into the surrounding air. Higher TEWL usually means the permeability barrier is leakier. TEWL is widely used in barrier research, but it is not a simple at-home diagnosis. Values depend on body site, temperature, humidity, device type, age, and protocol. A forehead number cannot be interpreted the same way as a lower-leg number.[2][8]
Filaggrin, natural moisturizing factors, and why eczema-prone skin is different
Filaggrin is a structural protein involved in epidermal differentiation and the formation of natural moisturizing factors. Loss-of-function mutations in the FLG gene are strongly linked with atopic dermatitis and a higher risk of dry, reactive, barrier-impaired skin. This does not mean every irritated face has a filaggrin mutation. It means barrier biology is real, genetic differences exist, and some people are easier to irritate than others.[5]
Skin pH and the acid mantle
Healthy skin surface pH is acidic, often around the high 4s to mid 5s, although values vary by site and method. This acidic environment helps support barrier enzymes, lipid processing, antimicrobial defense, and a balanced resident microbiome. Repeated use of high-pH soaps can shift the surface environment in a less barrier-friendly direction, which is one reason low-pH gentle cleansers are often better tolerated by reactive skin.[6]
The microbiome is part of the barrier story
Skin is colonized by microbes such as Staphylococcus epidermidis and Cutibacterium acnes. These organisms are not automatically enemies. In a balanced ecosystem, resident microbes can participate in immune education, pathogen resistance, and barrier defense. Problems arise when the barrier environment shifts, inflammation rises, or a specific organism overgrows in the wrong context.[7][11]
The same microbe can be normal in one context and involved in disease in another. Cutibacterium acnes can live on normal skin, but acne involves follicular plugging, sebum biology, immune activation, and strain-level differences, not simply having C. acnes on your face.
2. What damaged skin barrier means
A damaged barrier means the stratum corneum is not performing its protective and water-retaining role well. In research, this can show up as increased TEWL, altered hydration, lipid disruption, surface roughness, scaling, irritation, or increased response to irritants. In real life, it often feels like your skin has lost its tolerance.[1][2]
Common causes of barrier damage
- Over-exfoliation: frequent acids, scrubs, peels, or exfoliating toners can remove corneocytes faster than the skin can comfortably reorganize.
- Retinoid or benzoyl peroxide overuse: effective acne treatments can irritate when started too often, at too high a strength, or without moisturizer support.
- Harsh cleansing: high-pH soaps and strong surfactants can strip lipids, swell the stratum corneum, and worsen dryness.
- Alcohol-heavy or fragrance-heavy products: these are not automatically harmful for everyone, but they can be a problem for reactive or compromised skin.
- Environment: UV exposure, low humidity, wind, cold weather, pollution, hot water, and friction can all add stress.
- Skin disease: atopic dermatitis, rosacea, irritant dermatitis, allergic contact dermatitis, and acne treatment irritation can all involve barrier dysfunction.
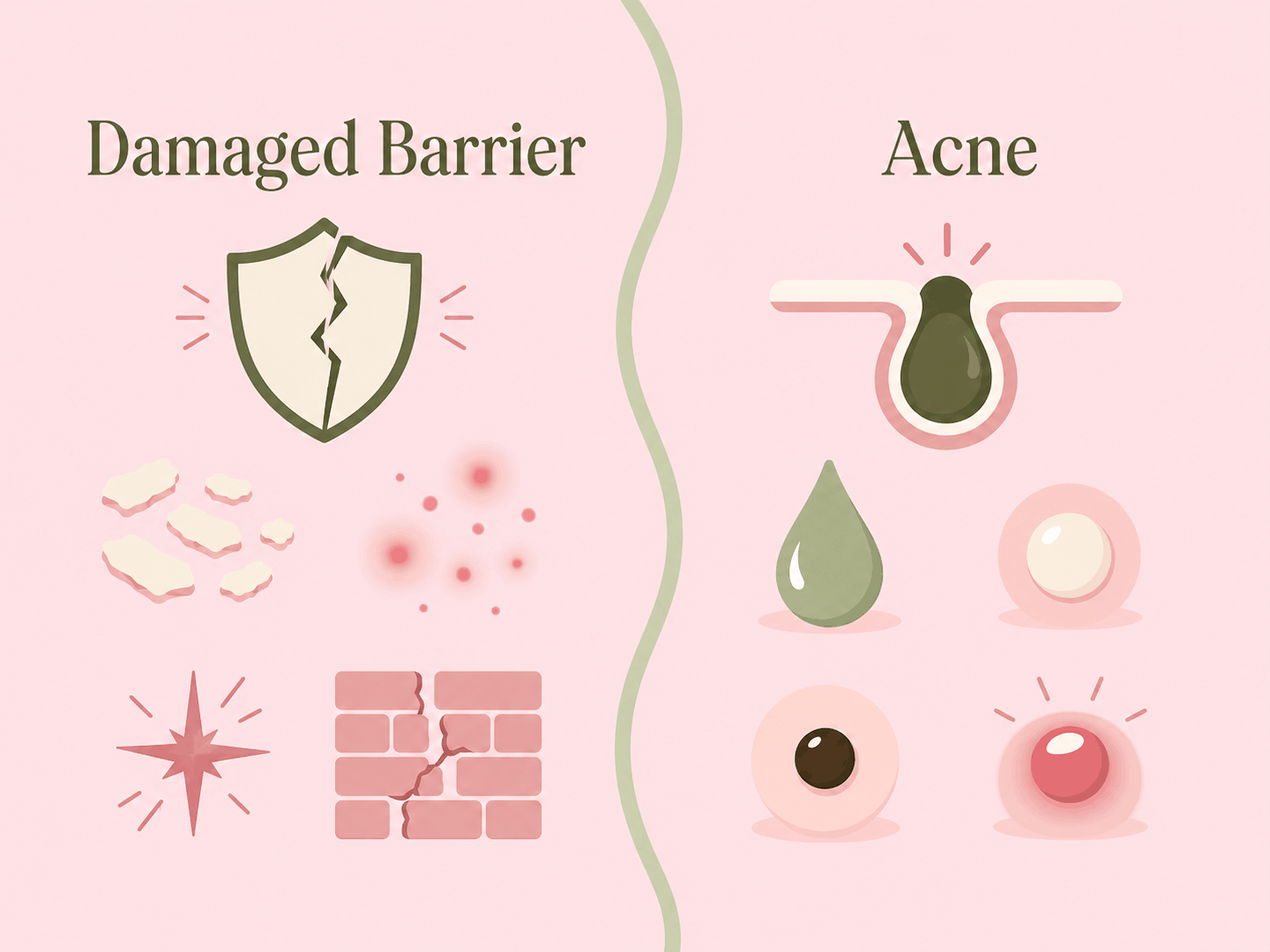
What barrier damage feels like
The classic signs are burning, stinging, tightness, roughness, flaking, redness, sensitivity, and sudden intolerance to products that used to be fine. A damaged barrier can also make acne look worse because inflammation and irritation can turn small bumps into angry-looking bumps.[1]
Inflammation is the bridge between barrier damage and acne-like bumps
Barrier disruption can trigger inflammatory signaling. The skin can release cytokines and activate repair pathways after injury. That inflammatory state can make the face look red, bumpy, and reactive. This is why a stripped face can look like it has acne even when the original problem was irritation, dermatitis, or over-treatment.[1][19]
Barrier damage can create acne-like breakouts, but that does not automatically make them true acne vulgaris. True acne usually includes follicular plugging and comedones. Irritant or acneiform eruptions often look more uniform, appear suddenly, and may lack blackheads and whiteheads.
3. What acne actually is
Acne vulgaris is a chronic inflammatory disease of the pilosebaceous unit. The core process is not simply dirty skin. It involves sebum production, abnormal follicular keratinization, Cutibacterium acnes activity, and inflammation. These mechanisms create comedones, papules, pustules, nodules, and cyst-like lesions.[11][12][13][14]
The four main acne mechanisms
Sebum production
Androgens stimulate sebaceous glands. More sebum can create a lipid-rich follicular environment that supports acne development.
Follicular plugging
Keratinocytes inside the follicle shed and stick abnormally, creating microcomedones that can become blackheads or whiteheads.
C. acnes signaling
C. acnes can contribute to inflammation through innate immune pathways, especially TLR2-related signaling.
Inflammation
Inflammation is present early in acne and drives redness, tenderness, papules, pustules, and deeper lesions.
Acne lesion types
DermNet describes acne lesions as centered on the pilosebaceous unit. Superficial lesions include open comedones, closed comedones, papules, and pustules. Deeper lesions include nodules and pseudocysts. Comedones are especially important because they point toward acne rather than simple barrier irritation.[17]
| Lesion | What it looks like | What it suggests |
|---|---|---|
| Open comedone | Blackhead or dark plug at the pore opening | Strong acne clue |
| Closed comedone | Small skin-colored or white bump under the surface | Strong acne clue |
| Papule | Small red tender bump | Can be acne, dermatitis, folliculitis, or irritation |
| Pustule | Inflamed bump with visible pus | Can be acne or folliculitis, context matters |
| Nodule | Deep painful lump | Strong inflammatory acne clue |
| Uniform itchy bumps | Many similar small follicular papules or pustules | Think acneiform eruption or Malassezia folliculitis too |
Hormonal acne
Hormonal acne is not a separate species of acne. It is acne in which androgen-sensitive sebum production and cyclical hormonal patterns are major drivers. It often appears around the lower face, jaw, chin, and cheeks, although location alone is not a diagnosis. Clues include recurring flares, deeper tender lesions, oily skin, and a pattern linked with menstrual cycles or androgen-related conditions.[11]
Diet and acne triggers
Acne triggers vary by person. Androgens, occlusion, stress, comedogenic exposure, and some dietary patterns can all matter in context. A randomized controlled trial by Smith et al. found that a low-glycemic-load diet improved acne symptoms compared with a control diet, which supports glycemic load as one possible acne-modifying factor. It does not prove that every breakout is caused by sugar or that diet replaces medical acne treatment.[11][16]
Malassezia folliculitis, often called fungal acne online
Malassezia folliculitis is not acne vulgaris. DermNet describes it as an infection of the pilosebaceous unit caused by lipophilic Malassezia yeasts. It often presents as small, uniform, itchy papules and pustules, especially on the upper back and chest, but it can involve the forehead, hairline, chin, neck, and upper limbs. Comedones are not seen, which helps distinguish it from acne vulgaris.[18]
4. Why barrier damage and acne get confused
They overlap because inflammation is visible. A damaged barrier can be red, bumpy, rough, shiny, flaky, and reactive. Acne can be red, bumpy, rough, oily, tender, and inflamed. The skin does not label each bump for you. You have to look for the pattern.
Barrier damage can mimic acne
Irritant dermatitis, allergic contact dermatitis, steroid acne, cosmetic reactions, mechanical acne, and acneiform eruptions can all resemble acne. NCBI's clinical summary notes that acneiform eruptions are often sudden, monomorphic, not always limited to sebaceous areas, and usually have fewer cysts than acne vulgaris.[19]
Acne treatments can damage the barrier
This is the trap. You see bumps, so you add salicylic acid. Then benzoyl peroxide. Then a retinoid. Then a scrub because the texture looks worse. Now the skin is inflamed, peeling, and burning, so every breakout looks more dramatic. Effective acne treatments can become counterproductive when the barrier is too irritated to tolerate them.[14]
Acne itself can impair barrier comfort
Acne-prone skin is not always a strong barrier skin type. Inflammation, frequent cleansing, drying acne medications, and picking can all increase sensitivity. Many people do not have either acne or barrier damage. They have acne plus a stressed barrier.
Burning, tightness, and flaking point toward barrier stress. Comedones and deep nodules point toward acne.
5. How to tell the difference
This is not a medical diagnosis, but it is a useful decision framework. Do not judge from one symptom. Judge from the cluster: timing, sensation, lesion type, location, and trigger.
| Clue | More like damaged barrier | More like acne | Could be both? |
|---|---|---|---|
| Timing | Sudden after a new product, over-exfoliation, retinoid increase, peel, harsh cleanser, or hot water | Recurring over weeks to months, often with repeated patterns | Yes, acne can worsen after aggressive treatment |
| Sensation | Burning, stinging, tight, hot, raw, or itchy | Usually tender only at lesions, not the whole face | Yes |
| Comedones | Often absent | Blackheads and whiteheads are major clues | Yes, acne with irritated barrier can still have comedones |
| Flaking | Common, especially with tightness | May happen from acne treatments or dryness | Very common |
| Distribution | Widespread, patchy, or exactly where a product was applied | Face, neck, chest, back, and sebaceous zones | Yes |
| Lesion shape | Uniform bumps, redness, roughness, or rash-like texture | Mixed lesion types: comedones, papules, pustules, nodules | Yes |
| Product tolerance | Even bland moisturizer or water can sting | Basic moisturizer usually does not burn | Yes, if acne treatment irritated the skin |
Signs that point more toward damaged barrier
- Your skin was mostly fine, then suddenly became reactive after a new product or over-treatment.
- Water, toner, moisturizer, sunscreen, or even sweat stings.
- Your face feels tight, shiny, hot, raw, or uncomfortable.
- There is widespread redness or sensitivity rather than individual pore-based lesions.
- Bumps appear all over in a similar pattern, not in your usual acne zones.
- You see flaking or rough patches at the same time as the bumps.
- There are few or no blackheads and whiteheads.
Signs that point more toward acne
- You have blackheads or closed comedones.
- You get deep, painful cyst-like lesions or nodules.
- Breakouts repeat in sebaceous zones such as the T-zone, chin, jaw, chest, or back.
- There is a hormonal pattern, such as flaring before menstruation.
- Your skin is oily and the breakouts are follicle-centered.
- Your basic moisturizer does not burn, even if acne spots are tender.
Signs you probably have both
- You clearly have acne lesions, but products now sting.
- Your acne worsened after starting benzoyl peroxide, retinoids, salicylic acid, peels, or scrubs too aggressively.
- You have comedones plus flaking, tightness, and rough irritated patches.
- You keep escalating actives because the bumps look worse, but the skin feels more inflamed each week.
Comedones tell you acne is involved. Burning tells you the barrier is involved.
That is the simplest useful rule6. How to treat each one without making it worse
If it looks like damaged barrier
Your goal is to reduce irritation and rebuild the lipid-water balance of the stratum corneum. That means fewer actives, gentler cleansing, more barrier support, and patience. The skin barrier can improve quickly when the trigger is removed, but full comfort may take longer depending on how irritated the skin is and whether there is underlying dermatitis or acne.
- Pause strong actives for 1 to 2 weeks: stop exfoliating acids, scrubs, peels, strong vitamin C, benzoyl peroxide, and retinoids until burning and tightness settle.
- Use a gentle cleanser: avoid high-pH soaps, aggressive foaming cleansers, and cleansing multiple times per day.
- Moisturize seriously: choose bland formulas with glycerin, ceramides, cholesterol, fatty acids, petrolatum, dimethicone, squalane, panthenol, or niacinamide if tolerated.
- Protect from UV: sunscreen matters because UV exposure is barrier stress and inflammation stress.
- Reintroduce slowly: once skin no longer burns, add only one active back at a time.
Ingredients that make sense for barrier repair
Ceramides, cholesterol, fatty acids
These match the lipid classes that help structure the stratum corneum barrier.
Glycerin, hyaluronic acid, urea
Humectants help hydration, but they are not enough alone if the skin is actively irritated.
Petrolatum, dimethicone
Occlusives reduce water loss and protect raw-feeling skin while it recovers.
Niacinamide, panthenol, colloidal oat
These can support comfort, but start cautiously if everything stings. Nicotinamide has evidence for increasing epidermal ceramide and other stratum corneum lipid biosynthesis in barrier research.[10]
Ceramide-containing moisturizers have evidence for improving dry skin signs and increasing stratum corneum lipid levels, but do not overstate the data. For example, Draelos et al. studied dry, itchy lower legs, not every type of facial irritation and not acne treatment failure. It is still useful evidence, just not magic proof for every barrier claim.[9]
If it looks like acne
Evidence-based acne treatment targets follicular plugging, C. acnes, sebum, and inflammation. The JAAD guidelines of care describe options such as benzoyl peroxide, topical retinoids, topical antibiotics used with benzoyl peroxide, salicylic acid, azelaic acid, oral antibiotics for appropriate inflammatory acne, hormonal therapies for appropriate patients, and isotretinoin for severe, scarring, or refractory acne. Systemic antibiotics should be limited to the shortest practical duration and paired with benzoyl peroxide or topical maintenance to reduce resistance risk.[15]
| Treatment | Main role | Barrier risk | How to use more intelligently |
|---|---|---|---|
| Benzoyl peroxide | Antimicrobial and anti-inflammatory acne treatment | Dryness, peeling, irritation | Try lower strengths, short-contact use, or every-other-day use if sensitive |
| Topical retinoid | Normalizes follicular keratinization and helps comedones | Retinoid dermatitis, peeling, burning | Use pea-sized amount, moisturize, start 2 to 3 nights weekly |
| Salicylic acid | Comedolytic BHA useful for oily, clogged skin | Overuse can irritate and dry skin | Use less often, avoid stacking with other exfoliants |
| Azelaic acid | Acne, redness, and post-inflammatory marks | Can sting at first | Start slowly, moisturize first if reactive |
| Oral antibiotics | Moderate inflammatory acne when needed | Resistance, side effects, microbiome impact | Use shortest practical duration with topical benzoyl peroxide and maintenance |
| Isotretinoin | Severe, scarring, or refractory acne | Strong dryness and irritation | Prescription only, requires medical monitoring |
7. What to do if you have acne and a damaged barrier
This is the most common real-world situation. The answer is not to quit acne treatment forever. The answer is to stop treating your face like a war zone.
Barrier-first does not mean ignoring acne. It means making the skin calm enough to tolerate acne treatment.
- Stabilize first: use a gentle cleanser, moisturizer, and sunscreen only until burning and tightness calm down.
- Keep acne treatment minimal: if acne is severe, do not DIY pause prescriptions without asking your clinician. If it is mild and self-treated, pause actives briefly.
- Restart one active: choose the one that matches your acne type. Retinoid for comedones, benzoyl peroxide for inflammatory lesions, salicylic acid for oily clogged texture.
- Use a buffer: apply moisturizer before retinoids or use a moisturizer sandwich if your skin is reactive.
- Do not stack everything: retinoid plus benzoyl peroxide plus acid plus scrub is how many people turn acne into acne plus dermatitis.
When to see a dermatologist
- You have painful nodules, cysts, or scarring.
- Your skin is swelling, crusting, oozing, or intensely itchy.
- Breakouts are sudden, uniform, itchy, and not responding to acne treatment.
- You suspect allergic contact dermatitis.
- You have acne that is affecting your mental health or confidence.
- You are using prescription acne treatment and your barrier feels destroyed.
FAQ
Can a damaged barrier cause acne?
It can worsen acne-looking inflammation and may contribute to breakouts indirectly, but true acne also involves follicular plugging, sebum biology, C. acnes activity, and inflammation. Barrier damage alone does not always equal acne.
How do I know if bumps are irritation or acne?
Look for comedones. Blackheads and whiteheads point toward acne. Burning, stinging, tightness, flaking, and sudden uniform bumps after product changes point toward barrier irritation.
Should I stop all acne products if my barrier is damaged?
If your acne is self-treated and mild, a short pause can help. If you are on prescription treatment or have severe acne, ask your dermatologist before stopping.
Is hyaluronic acid enough to repair the barrier?
No. Hyaluronic acid is a humectant. It helps hydration, but barrier repair usually needs lipid support, irritation reduction, and sometimes occlusive protection.
Can oily skin have a damaged barrier?
Yes. Oiliness and barrier strength are not the same thing. You can be oily, acne-prone, dehydrated, and irritated at the same time.
What is the fastest sign I overdid skincare?
Burning or stinging from products that should be bland is the red flag. If moisturizer, sunscreen, or water suddenly hurts, your barrier is likely irritated.
Acne is mostly identified by lesion type, especially comedones, recurring inflammatory lesions, and deeper nodules. Barrier damage is mostly identified by sensation, timing, and reactivity, especially burning, tightness, flaking, and sudden intolerance after product stress. When in doubt, calm the barrier first, then restart acne treatment slowly.
This article is for education only and is not a diagnosis. See a dermatologist for painful, scarring, spreading, infected, sudden, or treatment-resistant skin symptoms.
Stay picky with skincare,
Filip
Sources
Click to view all 19 sources
We prioritised peer-reviewed barrier biology papers, acne pathophysiology reviews, JAAD guidance, DermNet clinical references, and NCBI clinical summaries. Some older mechanistic papers are included because they remain foundational.
- [1] Proksch E, Brandner JM, Jensen JM. The skin: an indispensable barrier. Experimental Dermatology. 2008;17(12):1063-1072. doi: 10.1111/j.1600-0625.2008.00786.x.
- [2] Fluhr JW, Feingold KR, Elias PM. Transepidermal water loss reflects permeability barrier status: validation in human and rodent in vivo and ex vivo models. Experimental Dermatology. 2006;15(7):483-492. doi: 10.1111/j.1600-0625.2006.00437.x.
- [3] Elias PM. Stratum corneum defensive functions: an integrated view. Journal of Investigative Dermatology. 2005;125(2):183-200. doi: 10.1111/j.0022-202X.2005.23668.x.
- [4] Elias PM, Menon GK. Structural and lipid biochemical correlates of the epidermal permeability barrier. Advances in Lipid Research. 1991;24:1-26. doi: 10.1016/B978-0-12-024924-4.50005-5. PMID: 1763710.
- [5] Irvine AD, McLean WHI, Leung DYM. Filaggrin mutations associated with skin and allergic diseases. New England Journal of Medicine. 2011;365(14):1315-1327. doi: 10.1056/NEJMra1011040.
- [6] Lambers H, Piessens S, Bloem A, Pronk H, Finkel P. Natural skin surface pH is on average below 5, which is beneficial for its resident flora. International Journal of Cosmetic Science. 2006;28(5):359-370. doi: 10.1111/j.1467-2494.2006.00344.x.
- [7] Gallo RL, Nakatsuji T. Microbial symbiosis with the innate immune defense system of the skin. Journal of Investigative Dermatology. 2011;131(10):1974-1980. doi: 10.1038/jid.2011.182.
- [8] Kottner J, Lichterfeld A, Blume-Peytavi U. Transepidermal water loss in young and aged healthy humans: a systematic review and meta-analysis. Archives of Dermatological Research. 2013;305:315-323. doi: 10.1007/s00403-012-1313-6.
- [9] Draelos ZD, Baalbaki NH, Cook S, Raab S, Colon G. The effect of a ceramide-containing product on stratum corneum lipid levels in dry legs. Journal of Drugs in Dermatology. 2020;19(4):372-376. doi: 10.36849/JDD.2020.4796.
- [10] Tanno O, Ota Y, Kitamura N, Katsube T, Inoue S. Nicotinamide increases biosynthesis of ceramides as well as other stratum corneum lipids to improve the epidermal permeability barrier. British Journal of Dermatology. 2000;143(3):524-531. doi: 10.1111/j.1365-2133.2000.03705.x.
- [11] Moradi Tuchayi S, Makrantonaki E, Ganceviciene R, Dessinioti C, Feldman SR, Zouboulis CC. Acne vulgaris. Nature Reviews Disease Primers. 2015;1:15029. doi: 10.1038/nrdp.2015.29.
- [12] Zouboulis CC. Acne and sebaceous gland function. Clinics in Dermatology. 2004;22(5):360-366. doi: 10.1016/j.clindermatol.2004.03.004.
- [13] Kim J, Ochoa MT, Krutzik SR, Takeuchi O, Uematsu S, Legaspi AJ, et al. Activation of Toll-like receptor 2 in acne triggers inflammatory cytokine responses. The Journal of Immunology. 2002;169(3):1535-1541. doi: 10.4049/jimmunol.169.3.1535.
- [14] Nagy I, Pivarcsi A, Koreck A, et al. Distinct strains of Propionibacterium acnes induce selective human beta-defensin-2 and interleukin-8 expression in human keratinocytes through Toll-like receptors. Journal of Investigative Dermatology. 2005;124(5):931-938. doi: 10.1111/j.0022-202X.2005.23705.x.
- [15] Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. Journal of the American Academy of Dermatology. 2016;74(5):945-973.e33. doi: 10.1016/j.jaad.2015.12.037.
- [16] Smith RN, Mann NJ, Braue A, Makelainen H, Varigos GA. A low-glycemic-load diet improves symptoms in acne vulgaris patients: a randomized controlled trial. American Journal of Clinical Nutrition. 2007;86(1):107-115. doi: 10.1093/ajcn/86.1.107.
- [17] Oakley A, Ngan V, Morrison C, Jones C, Gupta M. Acne vulgaris. DermNet. Updated 2021. DermNet acne vulgaris.
- [18] Oakley A, Stewart T. Malassezia folliculitis. DermNet. Revised September 2020. DermNet Malassezia folliculitis.
- [19] Nair PA, Saleh HM, Salazar FJ. Acneiform eruptions. StatPearls. Treasure Island, FL: StatPearls Publishing. Last updated January 11, 2024. NCBI Bookshelf.