
If your cleanser suddenly burns, your moisturizer stings, and your skin feels tight even after applying three layers of hydration, your skin may not be "purging." It may be telling you that your routine pushed it past what it can tolerate.
The phrase "damaged skin barrier" gets thrown around online like it is one neat diagnosis. In dermatology, it is more accurate to think of it as a pattern of barrier dysfunction. It can overlap with irritant contact dermatitis, retinoid irritation, over-exfoliation, sensitive skin, eczema, rosacea, or even allergic contact dermatitis. Same vibe online. Very different management in real life.
A damaged skin barrier usually means the outer skin layer is losing water too easily and letting irritants bother the skin more than usual. The fix is not to buy ten "barrier repair" products. The fix is to stop the irritation cycle, rebuild with boring ingredients, and reintroduce actives slowly.
Table of Contents.
- What Your Skin Barrier Actually Is
- 9 Signs Your Routine Went Too Far
- What Damages the Barrier?
- Barrier Damage vs. Purging vs. Allergy
- The 7-Day Barrier Reset
- Ingredients That Actually Help
- What to Avoid While Healing
- How to Bring Actives Back
- When to See a Dermatologist
- Frequently Asked Questions
- Final Verdict
- Sources
What Your Skin Barrier Actually Is.
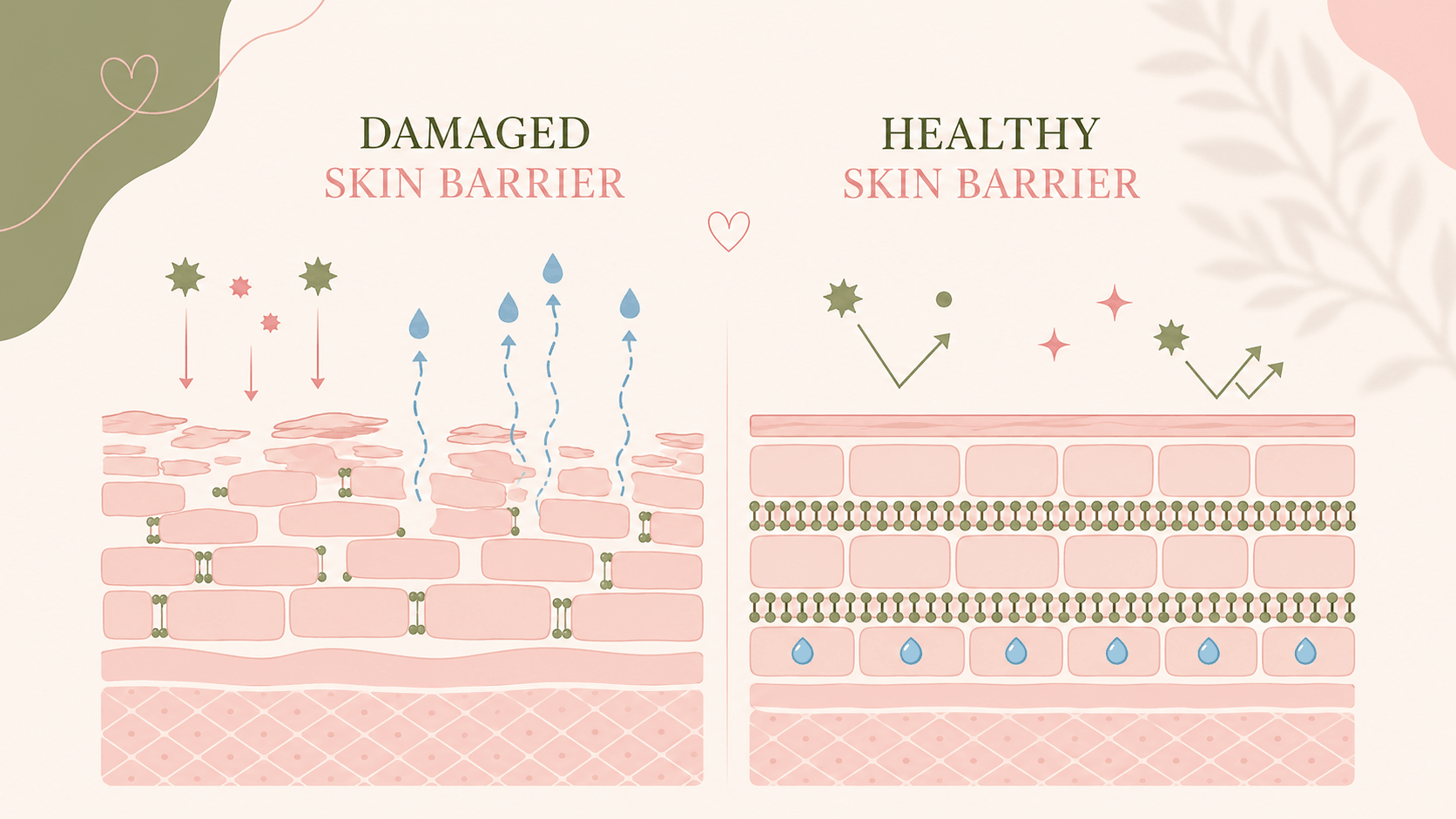
Your skin barrier is not just "dead skin." The main waterproofing layer is the stratum corneum, the outermost layer of the epidermis. Dermatologists often describe it like bricks and mortar: the "bricks" are flattened skin cells called corneocytes, and the "mortar" is a lipid matrix made mostly of ceramides, cholesterol, and free fatty acids. That lipid mix helps keep water in and irritants out.[1]
A healthy barrier also depends on natural moisturizing factor, which comes partly from filaggrin breakdown products. These water-binding molecules help the top skin layer stay flexible instead of dry, cracked, and reactive.[2] Below that, tight junctions act like another layer of control, helping regulate what passes between living skin cells.[3]
The barrier is a living system, not a trend word. It keeps water in, keeps irritants out, and helps the skin stay calm around microbes, weather changes, cleansing, and skincare actives.
When the barrier is disrupted, transepidermal water loss, often shortened to TEWL, tends to rise. That means more water escapes through the skin. The skin can feel tight, rough, shiny, flaky, or painfully dry, while products that used to feel normal suddenly sting. TEWL is used in research and clinical testing, but there is no single universal TEWL number that proves "your barrier is damaged" for every person, body site, or device.[4]
Skin barrier repair is mostly not glamorous. It is consistency, restraint, and the right boring ingredients.
That is why it works9 Signs Your Routine Went Too Far.
There is no validated "9 signs of damaged skin barrier" diagnostic score in dermatology. So think of this list as a practical pattern, not a medical diagnosis. The more signs you have, especially after adding acids, retinoids, benzoyl peroxide, scrubs, or a stronger cleanser, the more likely your routine is the problem.
A strong sign of a stressed barrier is stinging from products that are supposed to be bland. A mild tingle from an acid is one thing. Burning from water, moisturizer, or sunscreen is a different message.
Oiliness and dehydration can happen at the same time. Barrier disruption can increase water loss while your sebaceous glands still produce oil.
Redness can come from irritation, rosacea, allergy, eczema, or retinoid dermatitis. If it persists, spreads, or becomes swollen, stop guessing and get it checked.
Retinoids and exfoliating acids can increase shedding. A little dryness can happen. Patchy peeling with burning or tenderness suggests the routine is too aggressive.
When the stratum corneum is dehydrated and disorganized, skin may feel rough but look shiny. That shiny look is not always a glow.
Itch can appear with barrier disruption, but it also fits eczema, allergic contact dermatitis, and other skin conditions. Do not ignore persistent itch.
Benzoyl peroxide, salicylic acid, retinoids, and foaming cleansers can all be useful. But stacked together too often, they can create irritation that looks like more acne.
A compromised barrier can make even a good sunscreen sting. That does not always mean sunscreen is bad. It may mean your skin needs a simpler base routine first.
If your skin reacts to products it used to tolerate, your barrier reserve may be low, or you may have contact allergy, rosacea, eczema, or another condition that needs a different plan.
What Damages the Barrier?
Most barrier damage from skincare is cumulative. It is rarely one single product. It is usually the stack: a strong cleanser, exfoliating toner, vitamin C, retinoid, benzoyl peroxide spot treatment, clay mask, cleansing brush, and then panic-exfoliating again because texture looks worse.
| Trigger | What the science says |
|---|---|
| Harsh cleansing | Repeated washing and stronger surfactants can increase water loss, dryness, tightness, and irritation. Sodium lauryl sulfate is a classic research irritant used to model barrier disruption.[5] |
| Over-exfoliation | Acids are not automatically bad, but dose, pH, frequency, and layering matter. Chemical peels and microdermabrasion can temporarily disrupt barrier function, while lower-strength formulas may be tolerated better when used carefully.[6] Functional studies also show glycolic acid and retinoic acid can change stratum corneum properties, which is why frequency and tolerance matter.[7] |
| Retinoids | Retinoids can improve acne and photoaging, but early irritation is common. Burning, dryness, erythema, and peeling are recognized retinoid side effects, especially when started too often or layered with other irritants.[8] |
| Benzoyl peroxide | Benzoyl peroxide can be very useful for acne, but it can also be drying or irritating in real routines. Acne-prone skin may already show altered barrier parameters, so drying acne-treatment stacks can be harder to tolerate when the routine is too aggressive.[9] |
| Scrubs, brushes, and rough towels | Mechanical friction can remove or disturb the stratum corneum faster than it repairs. Tape stripping is literally used in studies to create a controlled barrier-disruption model.[10] |
| Low humidity and cold weather | Low humidity and lower temperatures are linked with weaker barrier function and more susceptibility to mechanical irritation. That is why a routine can feel fine in summer and rude in winter.[11] |
| Fragrance and allergens | Sometimes the issue is not just irritation. Allergic contact dermatitis can mimic a damaged barrier and may require patch testing, especially when symptoms repeat or localize around product use.[12] |
If you are rebuilding your routine, start with the basics: learn how to use salicylic acid without damaging your skin barrier, read our full review of The Ordinary Glycolic Acid 7%, and choose a simple base from our guide to the best moisturizers for oily, acne-prone skin.
"My skin hates everything" usually means one of three things: the barrier is irritated, the skin is inflamed from a condition like rosacea or eczema, or there is a contact allergy. The treatment path changes depending on which one is true.
Barrier Damage vs. Purging vs. Allergy.
This is where social media gets messy. Not every breakout after a new active is purging. Not every burning face is a damaged barrier. And not every "repair cream" is safe for every sensitive person.
Small acne lesions in areas where you usually break out, starting after an active that increases cell turnover, such as a retinoid or exfoliating acid. It should not feel like your whole face is on fire.
Burning, stinging, tightness, peeling, redness, tenderness, and reacting to bland products, especially after too many actives, over-cleansing, or exfoliation.
Itchy rash, swelling, eyelid involvement, sharply patterned reactions, or repeated flares after the same product type. This may need patch testing.
Burning, flushing, persistent redness, scaling, or recurrent itchy patches that come back even with a simple routine. Do not keep forcing actives through this.
A good rule: if your skin is burning and getting more reactive, do not call it purging just because you want the product to work. Purging should not make basic skincare feel painful.
The 7-Day Barrier Reset.
This is a conservative, dermatologist-style reset. It is not magic, and it is not a cure for every rash. But for routine-induced irritation, it removes the usual triggers and gives the barrier a chance to recover.
Retinoids, exfoliating acids, benzoyl peroxide, scrubs, cleansing brushes, peel pads, vitamin C if it stings, fragranced products, clay masks, alcohol-heavy toners, and any "tingly" product you are using just because TikTok said it works.
Go boring immediately
Use lukewarm water or a very gentle cleanser. Apply a bland moisturizer while the skin is slightly damp. Use sunscreen in the morning if you are exposed to daylight.
Stop testing new products
This is not the week to try a viral serum. Keep the routine identical so you can tell whether your skin is calming down.
Use moisturizer like treatment
Look for a formula with humectants, emollients, and occlusives. If small areas are cracked or painfully dry, a thin layer of petrolatum on top can help reduce water loss.
Check the direction
Improvement matters more than perfection. Less stinging, less tightness, and better comfort with moisturizer are good signs.
Do not rush actives back
The classic mistake is feeling 40% better and immediately using retinol again. Wait until water, cleanser, moisturizer, and sunscreen feel comfortable.
Keep sunscreen practical
If your usual SPF stings, choose the blandest sunscreen you tolerate. Daily UV protection still matters because UV exposure can worsen inflammation and barrier stress.
Plan the restart, not the comeback tour
When the skin is calm, reintroduce one active at a time. Your old routine may have been too much, even if every product was "good" on its own.
Ingredients That Actually Help.
A good barrier repair product does not need to sound rare or expensive. The strongest formulas usually combine three types of ingredients: humectants to hold water, emollients to smooth, and occlusives to reduce water loss. Emollients and moisturizers have the strongest practical evidence base in eczema-style barrier care, even though the best product still depends on tolerance and skin condition.[19] If your skin is oily or acne-prone, our guide to barrier-friendly moisturizers for oily, acne-prone skin is a good next read.
Petrolatum is one of the best-supported ingredients for reducing water loss. It is not glamorous, but it is extremely useful when skin is cracked, stinging, or very dry. Use a thin layer, especially at night or on irritated patches.[13]
Ceramides are important, but the barrier uses a lipid system. Research supports the idea that physiologic lipid mixtures are more barrier-logical than single-ingredient hype.[14]
Glycerin helps increase stratum corneum hydration and has evidence for supporting barrier recovery. It is one of the most reliable boring ingredients in skincare.[15]
Dexpanthenol has clinical evidence for improving hydration, reducing roughness, and supporting barrier repair after irritation models.[16]
Niacinamide can support barrier function and help with uneven tone. But if your skin currently stings from everything, even niacinamide may feel like too much at first. Add it back when the skin is calmer.[17]
Useful in many dry, itchy, eczema-prone routines. It is not required, but it can be a nice support ingredient if you tolerate it well.
Good for hydration, but not enough by itself. In a damaged barrier phase, hyaluronic acid works best inside a complete moisturizer, not as a watery serum under nothing.
Low percentages can be moisturizing. Higher percentages can feel keratolytic and may sting on compromised facial skin. Save stronger urea formulas for body areas unless advised otherwise.
What to Avoid While Healing.
Peeling skin makes people want to exfoliate. That usually resets the irritation loop. Moisturize instead.
Three new "barrier serums" can irritate more than one boring cream. Fewer variables is smarter.
Use a gentle cleanser and be patient. Over-cleansing at night can undo the repair work.
If one area keeps flaring or your eyelids react, patch testing may be more useful than another moisturizer.
How to Bring Actives Back.
Once your skin no longer stings with water, cleanser, moisturizer, or sunscreen, you can think about actives again. Not all at once. One.
| Active | Smarter restart |
|---|---|
| Retinoid | Restart 1 to 2 nights per week. Use moisturizer before or after if needed. Increase only after one to two weeks of comfort. |
| AHA or BHA exfoliant | Restart once weekly at first. Do not use on the same night as retinoid while rebuilding tolerance. For ingredient-specific guidance, see our guides to salicylic acid and The Ordinary Glycolic Acid 7%. |
| Benzoyl peroxide | Consider short-contact use, lower frequency, or applying only to acne-prone zones. Moisturizer matters. |
| Vitamin C | If acidic L-ascorbic acid stings, wait longer or use a gentler formula. Brightening is not urgent if your face is burning. |
| Clay masks and scrubs | These are optional, not skincare essentials. If your barrier keeps crashing, leave them out. |
You do not need a stronger routine. You need a routine your skin can survive long enough to benefit from.
When to See a Dermatologist.
See a dermatologist or qualified clinician if your skin is getting worse despite stopping actives, if symptoms last longer than one to two weeks, if you have swelling, crusting, oozing, severe pain, eye involvement, recurrent eyelid dermatitis, or a rash that keeps returning in the same pattern.
Patch testing is especially important when allergic contact dermatitis is possible. Biopsy is usually not the first tool for routine barrier irritation, and research shows skin biopsy is not reliable for cleanly separating allergic contact dermatitis, irritant contact dermatitis, and atopic dermatitis in many cases.[18]
Frequently Asked Questions.
How long does it take to heal a damaged skin barrier?
Mild irritation often improves within a few days to a week of simplifying your routine. More significant barrier disruption can take two to four weeks. If there is no improvement after two weeks, see a dermatologist.
Can a damaged skin barrier heal itself?
Yes, in most cases. The skin barrier is designed to repair itself once the irritating triggers are removed and it is given consistent, gentle care.
Is it bad to moisturize a damaged skin barrier too much?
Over-layering multiple "repair" products at once can itself become an irritant. One consistent, simple moisturizer is usually more effective than several at once.
What ingredients should I avoid with a damaged skin barrier?
Avoid retinoids, exfoliating acids, benzoyl peroxide, fragrance, alcohol-based toners, and physical scrubs until the barrier has recovered.
Final Verdict.
The most science-true way to repair a stressed barrier is boring: stop the triggers, cleanse gently, moisturize with a complete barrier-supportive formula, protect with sunscreen, and reintroduce actives slowly. The mistake is treating irritation like a problem that needs more products.
If your skin is burning, tight, peeling, and suddenly angry at everything, do not panic-buy. Simplify. Let the outer layer recover. Then build a routine that respects your skin instead of constantly testing how much it can take.
Pretty skin is not irritated skin pretending to glow.
This article is for educational purposes only and does not replace medical advice. If you have severe, persistent, painful, infected, swollen, or eye-area symptoms, speak with a dermatologist or qualified clinician.
Sources
Click to view all 19 sources
Literature cited in the article. We prioritized peer-reviewed studies, PubMed or PMC-indexed reviews, Cochrane evidence, and dermatology organization guidance.
- [1] Berdyshev E. Skin Lipid Barrier: Structure, Function and Metabolism. Allergy Asthma Immunol Res. 2024 Sep;16(5):445-461. doi: 10.4168/aair.2024.16.5.445. PMID: 39363765; PMCID: PMC11450438.
- [2] Hoste E, Kemperman P, Devos M, Denecker G, Kezic S, Yau N, Gilbert B, Lippens S, De Groote P, Roelandt R, Van Damme P, Gevaert K, Presland RB, Takahara H, Puppels G, Caspers P, Vandenabeele P, Declercq W. Caspase-14 is required for filaggrin degradation to natural moisturizing factors in the skin. J Invest Dermatol. 2011 Nov;131(11):2233-41. doi: 10.1038/jid.2011.153. Epub 2011 Jun 9. PMID: 21654840.
- [3] Kirschner N, Houdek P, Fromm M, Moll I, Brandner JM. Tight junctions form a barrier in human epidermis. Eur J Cell Biol. 2010 Nov;89(11):839-42. doi: 10.1016/j.ejcb.2010.07.010. Epub 2010 Aug 21. PMID: 20732726.
- [4] Akdeniz M, Gabriel S, Lichterfeld-Kottner A, Blume-Peytavi U, Kottner J. Transepidermal water loss in healthy adults: a systematic review and meta-analysis update. Br J Dermatol. 2018 Nov;179(5):1049-1055. doi: 10.1111/bjd.17025. Epub 2018 Sep 9. PMID: 30022486.
- [5] Tupker RA, Pinnagoda J, Nater JP. The transient and cumulative effect of sodium lauryl sulphate on the epidermal barrier assessed by transepidermal water loss: inter-individual variation. Acta Derm Venereol. 1990;70(1):1-5. PMID: 1967864.
- [6] Fartasch M, Teal J, Menon GK. Mode of action of glycolic acid on human stratum corneum: ultrastructural and functional evaluation of the epidermal barrier. Arch Dermatol Res. 1997 Jun;289(7):404-9. doi: 10.1007/s004030050212. PMID: 9248619.
- [7] Effendy I, Kwangsukstith C, Lee JY, Maibach HI. Functional changes in human stratum corneum induced by topical glycolic acid: comparison with all-trans retinoic acid. Acta Derm Venereol. 1995 Nov;75(6):455-8. doi: 10.2340/0001555575455458. PMID: 8651024.
- [8] Motamedi M, Chehade A, Sanghera R, Grewal P. A Clinician's Guide to Topical Retinoids. J Cutan Med Surg. 2022 Jan-Feb;26(1):71-78. doi: 10.1177/12034754211035091. Epub 2021 Jul 22. PMID: 34292058; PMCID: PMC8750127.
- [9] Sukanjanapong S, Ploydaeng M, Wattanakrai P. Skin Barrier Parameters in Acne Vulgaris versus Normal Controls: A Cross-Sectional Analytic Study. Clin Cosmet Investig Dermatol. 2024 Nov 1;17:2427-2436. doi: 10.2147/CCID.S476004. PMID: 39502708; PMCID: PMC11537166.
- [10] Breternitz M, Flach M, Prässler J, Elsner P, Fluhr JW. Acute barrier disruption by adhesive tapes is influenced by pressure, time and anatomical location: integrity and cohesion assessed by sequential tape stripping. A randomized, controlled study. Br J Dermatol. 2007 Feb;156(2):231-40. doi: 10.1111/j.1365-2133.2006.07632.x. PMID: 17223861.
- [11] Engebretsen KA, Johansen JD, Kezic S, Linneberg A, Thyssen JP. The effect of environmental humidity and temperature on skin barrier function and dermatitis. J Eur Acad Dermatol Venereol. 2016 Feb;30(2):223-49. doi: 10.1111/jdv.13301. Epub 2015 Oct 8. PMID: 26449379.
- [12] British Association of Dermatologists. (2024, July). Patch testing.
- [13] Czarnowicki T, Malajian D, Khattri S, Correa da Rosa J, Dutt R, Finney R, Dhingra N, Xiangyu P, Xu H, Estrada YD, Zheng X, Gilleaudeau P, Sullivan-Whalen M, Suaréz-Fariñas M, Shemer A, Krueger JG, Guttman-Yassky E. Petrolatum: Barrier repair and antimicrobial responses underlying this "inert" moisturizer. J Allergy Clin Immunol. 2016 Apr;137(4):1091-1102.e7. doi: 10.1016/j.jaci.2015.08.013. Epub 2015 Oct 1. PMID: 26431582.
- [14] Man MQ M, Feingold KR, Thornfeldt CR, Elias PM. Optimization of physiological lipid mixtures for barrier repair. J Invest Dermatol. 1996 May;106(5):1096-101. doi: 10.1111/1523-1747.ep12340135. PMID: 8618046.
- [15] Fluhr JW, Gloor M, Lehmann L, Lazzerini S, Distante F, Berardesca E. Glycerol accelerates recovery of barrier function in vivo. Acta Derm Venereol. 1999 Nov;79(6):418-21. doi: 10.1080/000155599750009825. PMID: 10598752.
- [16] Proksch E, Nissen HP. Dexpanthenol enhances skin barrier repair and reduces inflammation after sodium lauryl sulphate-induced irritation. J Dermatolog Treat. 2002 Dec;13(4):173-8. doi: 10.1080/09546630212345674. PMID: 19753737.
- [17] Mohammed D, Crowther JM, Matts PJ, Hadgraft J, Lane ME. Influence of niacinamide containing formulations on the molecular and biophysical properties of the stratum corneum. Int J Pharm. 2013 Jan 30;441(1-2):192-201. doi: 10.1016/j.ijpharm.2012.11.043. Epub 2012 Dec 5. PMID: 23220080.
- [18] Frings VG, Böer-Auer A, Breuer K. Histomorphology and Immunophenotype of Eczematous Skin Lesions Revisited-Skin Biopsies Are Not Reliable in Differentiating Allergic Contact Dermatitis, Irritant Contact Dermatitis, and Atopic Dermatitis. Am J Dermatopathol. 2018 Jan;40(1):7-16. doi: 10.1097/DAD.0000000000000842. PMID: 28296664.
- [19] van Zuuren EJ, Fedorowicz Z, Christensen R, Lavrijsen A, Arents BWM. Emollients and moisturisers for eczema. Cochrane Database Syst Rev. 2017 Feb 6;2(2):CD012119. doi: 10.1002/14651858.CD012119.pub2. PMID: 28166390; PMCID: PMC6464068.