
A pimple heals, the redness calms down, and then another bump appears in the same little area. It can feel like one pore is broken forever.
The more accurate answer is less dramatic. Acne can keep returning to the same small zone, but the evidence does not prove that one exact follicle is always reactivating. It may be the same follicle, a nearby follicle, or the same acne-prone patch of skin responding to the same conditions again.[1][2][5]
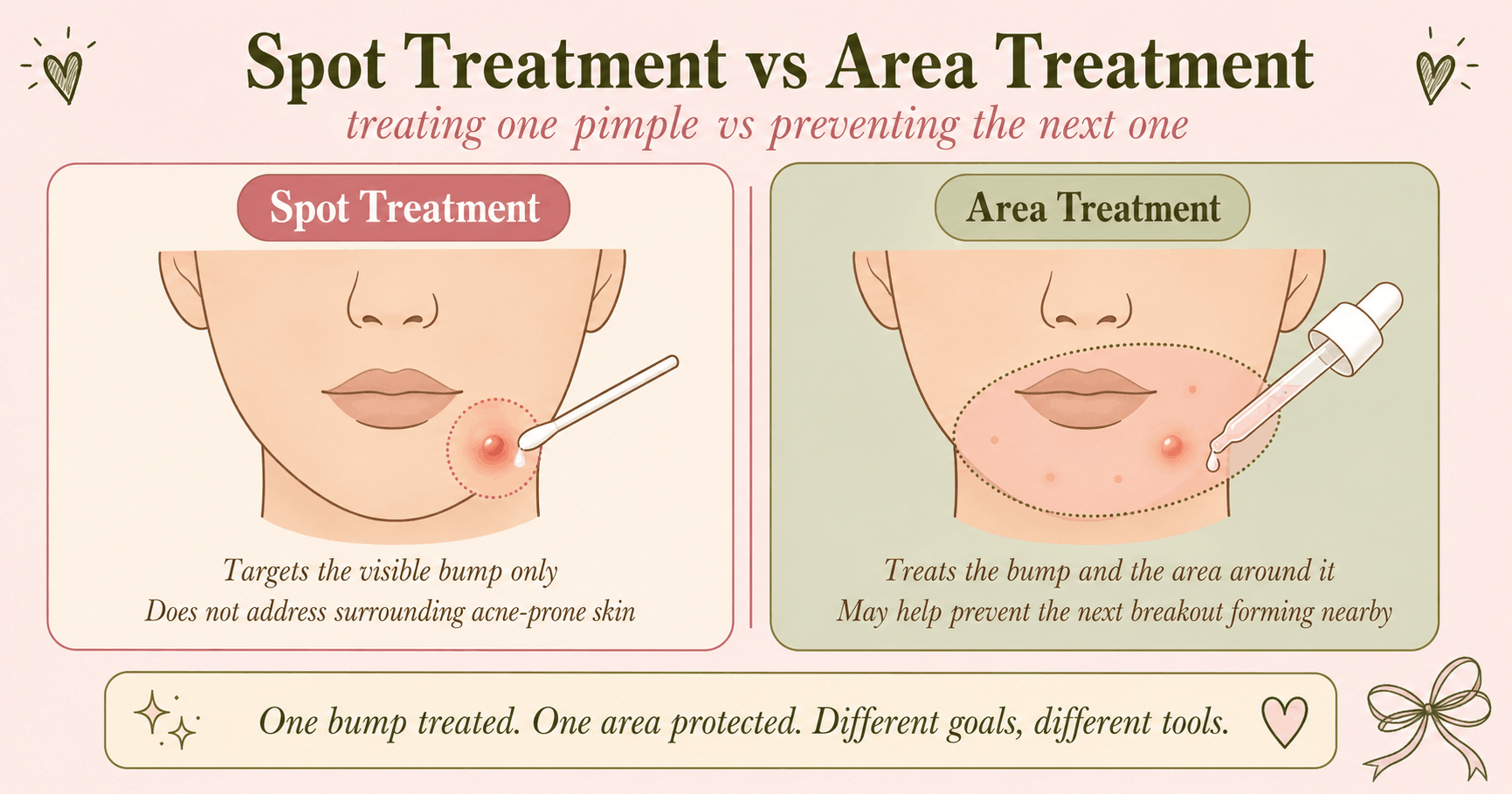
Recurring acne in one small area can reflect skin that is still acne-prone, not a scar that is trapping oil forever. Ongoing microcomedo formation, sebum, inflammation, hormones, friction, occlusion, or repeated product contact may keep the same area active. These factors can sustain acne in a region, but research has not shown that they explain every lesion that appears to return in the exact same spot. Spot treatment can calm a visible bump, but prevention often has to cover the acne-prone area.
Table of Contents
What “same spot” really means
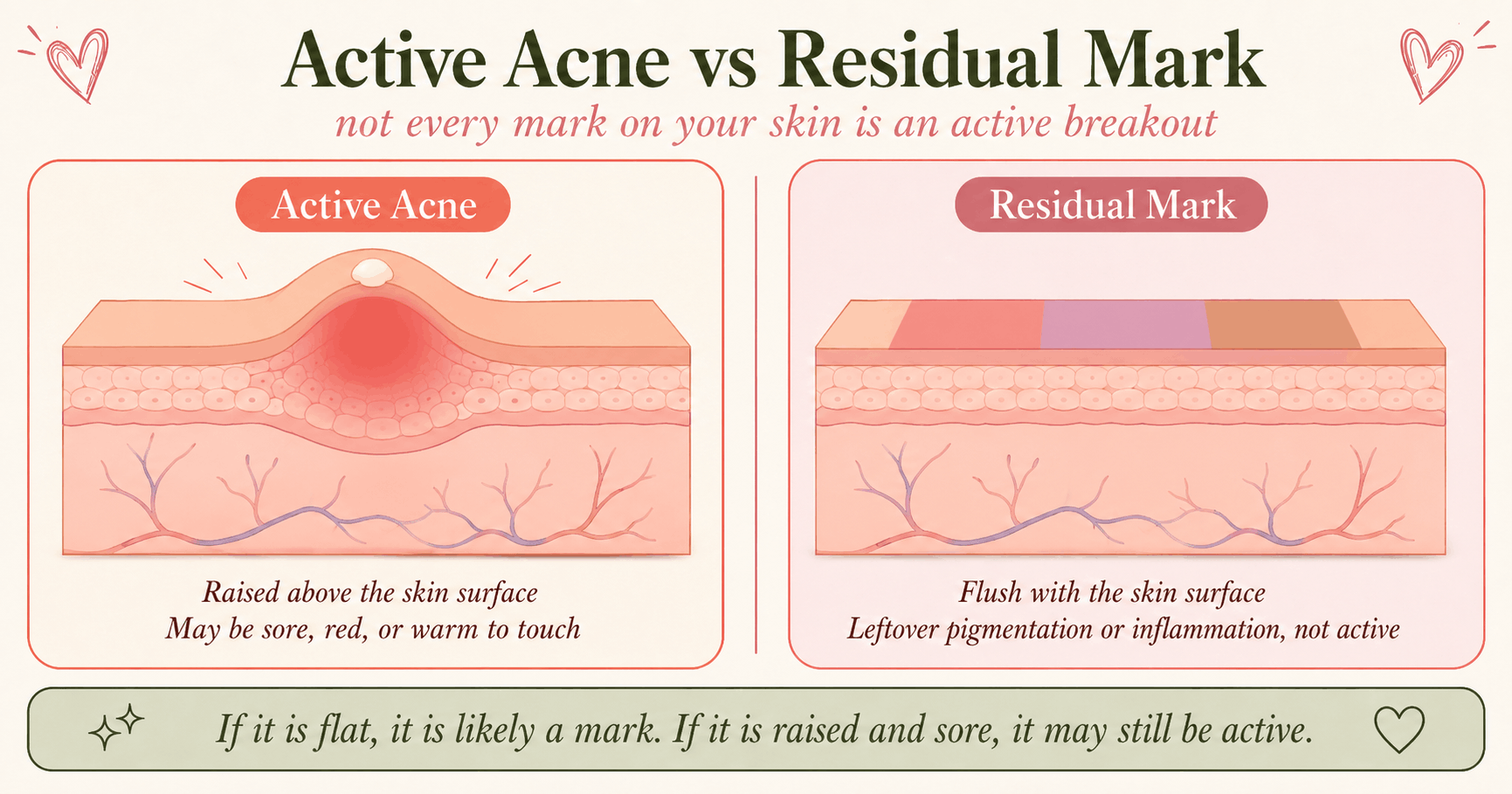
The visible inflammation around a pimple can extend beyond the follicular opening. The redness, swelling, and leftover color can cover a small area of skin. So when another bump appears close by, it can look like the exact same pimple came back.
A flat red, purple, or brown mark is often leftover inflammation or pigmentation after acne. Still, color alone is not enough to diagnose it. If the area becomes raised, sore, swollen, or forms a whitehead, it may be active again. If it stays flat and slowly fades, it is more likely a residual mark than a new clogged pore.[3][13]
Why acne can return in one area
1. Acne often starts before you can see it
A useful prevention-focused explanation is microcomedo formation. A microcomedo is an early, invisible clogged follicle linked to abnormal follicular shedding, sebum, inflammation, and microbial changes before a red bump appears.[1]
That does not mean one microcomedo lives forever. A better way to say it is this: the same area may keep forming new microcomedones if the local conditions do not change. This is a reasonable prevention argument, not direct proof that every repeat bump comes from the exact same follicle.
2. The same trigger keeps touching the same skin
Friction, pressure, and occlusion can keep one area active. Helmets, chin straps, tight gear, and some hair products can repeatedly affect the same skin. Repeated friction or occlusion from habits or objects touching the same area may also contribute in some people. Acne mechanica is recognized, and AAD patient guidance specifically discusses sports equipment and hair-care products as acne triggers. Cell-phone acne is much weaker evidence, so it should not be treated as a common proven cause.[6][7][17][18]
3. Hormones can keep a region sensitive
Jawline and lower-face acne can be hormonally influenced, especially in adult women, but not every jawline breakout is hormonal. AAD patient guidance notes that women with acne along the lower face, jawline, and neck may respond well to hormonal therapy. The AAD guideline also supports treatment categories such as benzoyl peroxide, topical retinoids, azelaic acid, salicylic acid, clascoterone, oral antibiotics when appropriate, combined oral contraceptives, spironolactone, and isotretinoin for selected patients.[4][9][14][19]
4. Treatment stops too early
This can happen: the bump improves, so the treatment stops. But the invisible acne process may still be active around it. That is why acne prevention is usually about treating the acne-prone area as directed, not just the center of one spot.
What is not proven
| Claim | Better science-backed wording |
|---|---|
| “The same pore is infected forever.” | Not proven. The same small area may keep forming acne, but exact-follicle recurrence has not been clearly demonstrated by the cited sources. |
| “An acne scar causes the next pimple.” | Acne can lead to scarring, and longer inflammation increases risk, but that does not prove a scar causes new acne.[3] |
| “If it burns, it is working.” | No. Irritation is not required. Significant irritation can make treatment harder to tolerate and use consistently. More irritation does not mean better or faster results. |
| “A pimple patch prevents recurrence.” | A hydrocolloid patch can protect a suitable superficial lesion and may support healing, but standard patches are not established treatment for preventing future microcomedones or recurring acne. |
| “Biofilm explains every repeat spot.” | Biofilms are an interesting acne research area, but they do not prove that every recurring pimple comes from one permanently infected pore.[12] |
How to stop acne from returning in the same area
The main strategy is simple: treat the zone before the next bump becomes visible.
Our evidence assessment: strongly guideline-aligned for area-directed prevention. This is an editorial evidence assessment, not a formal GRADE rating. Spot treatment alone: supplemental. It can help a visible bump, but it is not a full prevention plan. Expected speed: gradual. NICE says improvement may take 6 to 8 weeks, and many first-line courses are reviewed at 12 weeks.[8]
Depending on acne severity and individual factors, guideline-supported treatment options include a topical retinoid, benzoyl peroxide, azelaic acid, salicylic acid, or combination treatment. Clascoterone is applied over the affected area, not as a tiny spot treatment, for best efficacy in the clinical review.[10]
Use treatment gently enough to stay consistent. More burning does not mean faster results. If significant irritation develops, reduce frequency, use a gradual or short-contact approach when appropriate, and seek professional advice if symptoms are severe or persistent.
Pregnancy matters. NICE states that topical retinoids and oral tetracyclines are contraindicated during pregnancy and when planning pregnancy. Oral isotretinoin must not be used during pregnancy and is subject to strict pregnancy-prevention requirements. Ask a clinician before using acne medication in that situation.[8]
Maintenance can matter if acne relapses often. NICE specifically recommends considering fixed adapalene plus benzoyl peroxide as a maintenance option for people with frequent relapse when suitable. The maintenance trial behind this type of approach involved severe-acne patients who had already improved and was sponsored by the manufacturer connected to the tested product, so the context should be kept in mind.[8][11]
A simple recurring-acne routine
Morning
- Cleanse gently up to twice daily, adjusting if irritation develops.
- Use a light, non-comedogenic moisturizer if your skin feels dry.
- Apply broad-spectrum SPF 30 or higher, especially when using acne treatments that increase sun sensitivity.[13]
Evening
- Cleanse gently after significant sweating, sunscreen, makeup, or buildup from occlusive gear.
- Apply your preventive acne treatment to the acne-prone area as directed, not only the visible center of one bump.
- A hydrocolloid patch can protect a suitable superficial lesion and may support healing, but standard patches are not established treatment for preventing future microcomedones or recurring acne.
- Introduce new active treatments gradually rather than starting several at once. Consistency beats a chaotic routine.
When a recurring bump may not be acne
If one “pimple” keeps returning in exactly the same place, gets deep and painful, drains repeatedly, leaves scars, or never fully goes away, get it checked. Other possibilities include folliculitis, perioral dermatitis, or hidradenitis suppurativa. A persistent isolated lump may represent another condition and should be assessed. Hidradenitis suppurativa most often affects skin-fold areas such as the armpits, inner thighs, and groin, so it should not be framed as an ordinary recurrent facial pimple.[16][20]
Also get help for severe, scarring, sudden, or emotionally distressing acne. Isotretinoin can be highly effective for selected patients, but relapse is possible. In one US commercial-claims cohort of 19,907 patients with at least one year of post-treatment enrolment, 22.5% met the study’s claims-based definition of relapse and 8.2% had another isotretinoin course during follow-up. Those are not lifetime relapse numbers.[15]
Do not chase the same pimple forever. Treat the acne-prone area that keeps making new ones.
That is the practical takeaway.FAQ
Why does acne keep coming back in the same spot?
The area may still be acne-prone. Ongoing microcomedo formation, oil, inflammation, friction, hormones, or repeated product contact can keep triggering new lesions nearby.
Is it always the exact same pore?
No. It might be the same follicle, but it could also be a nearby follicle in the same small zone. The evidence does not prove exact-follicle recurrence in most cases.
Is a flat red or brown mark active acne?
It is often a residual mark, but watch the texture. If it becomes raised, sore, swollen, or forms a head, it may be active again.
Does acne treatment need to irritate my skin?
No. Irritation is not required. Significant irritation can make treatment harder to tolerate and use consistently.
Do pimple patches stop recurring acne?
A hydrocolloid patch can protect a suitable superficial lesion and may support healing, but standard patches are not established treatment for preventing future microcomedones or recurring acne.
How long should I give a routine?
Expect weeks, not days. NICE says improvement may take 6 to 8 weeks, and many first-line treatments are reviewed at 12 weeks.
When should I see a dermatologist?
See one for deep painful lumps, scarring, sudden severe acne, repeated painful lumps, or acne that does not improve after consistent treatment.
References
- Xie L, Hamblin MR, Zheng DL, Wen X. The role of microcomedones in acne: Moving from a description to treatment target? J Dtsch Dermatol Ges. 2024;22(1):9-16. doi: 10.1111/ddg.15272. PMID: 38123894. Available from: PubMed.
- Josse G, Mias C, Le Digabel J, et al. High bacterial colonization and lipase activity in microcomedones. Exp Dermatol. 2020;29(2):168-176. doi: 10.1111/exd.14069. PMID: 31863492. Mechanistic study of sampled microcomedones, not a recurrence study. Most authors were affiliated with Pierre Fabre Laboratories' Skin Research Center; the authors declared no conflicts of interest. Available from: PubMed.
- Tan J, Bourdès V, Bissonnette R, et al. Prospective Study of Pathogenesis of Atrophic Acne Scars and Role of Macular Erythema. J Drugs Dermatol. 2017;16(6):566-572. PMID: 28686774. This source supports acne-related erythema and scarring context, not proof that pigmentation commonly creates apparent same-site recurrence. Available from: PubMed.
- Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90(5):1006.e1-1006.e30. doi: 10.1016/j.jaad.2023.12.017. PMID: 38300170. Available from: PubMed.
- Yu T, Xu X, Liu Y, et al. Multi-omics signatures reveal genomic and functional heterogeneity of Cutibacterium acnes in normal and diseased skin. Cell Host Microbe. 2024;32(7):1129-1146.e8. doi: 10.1016/j.chom.2024.06.002. PMID: 38936370. Relevant to C. acnes biology and genomic and functional heterogeneity, not direct proof of exact-location acne recurrence. Available from: PubMed.
- Mazhar M, Simpson M, Marathe K. Inner thigh friction as a cause of acne mechanica. Pediatr Dermatol. 2019;36(4):546-547. doi: 10.1111/pde.13817. PMID: 30883890. Single case report, useful for the clinical concept but not broad causal estimates. Available from: PubMed.
- Singh M, Pawar M, Maheswari A, Bothra A, Khunger N. 'Cell-phone acne' epidemic during the COVID-19 pandemic. Clin Exp Dermatol. 2020;45(7):903-905. doi: 10.1111/ced.14360. PMID: 32598514; PMCID: PMC7362163. Letter; useful as a limited clinical observation, not strong evidence of prevalence or causality. Available from: PubMed Central.
- National Institute for Health and Care Excellence. Acne vulgaris: management. NICE guideline NG198. Published June 25, 2021. Last updated April 30, 2026. Available from: NICE.
- American Academy of Dermatology Association. Acne clinical guideline. Guideline highlights and treatment recommendations. Accessed July 14, 2026. Available from: AAD.
- Canadian Agency for Drugs and Technologies in Health. Clascoterone (Winlevi): Therapeutic area: Acne vulgaris: Reimbursement Review [Internet]. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2025 Jun. Clinical Review. NCBI Bookshelf. Available from: NCBI Bookshelf.
- Poulin Y, Sanchez NP, Bucko A, et al. A 6-month maintenance therapy with adapalene-benzoyl peroxide gel prevents relapse and continuously improves efficacy among patients with severe acne vulgaris: results of a randomized controlled trial. Br J Dermatol. 2011;164(6):1376-1382. doi: 10.1111/j.1365-2133.2011.10344.x. PMID: 21457209. Randomized vehicle-controlled maintenance trial in 243 severe-acne responders. The study was supported by Galderma R&D; two authors were Galderma R&D employees. Available from: PubMed.
- Jahns AC, Lundskog B, Ganceviciene R, et al. An increased incidence of Propionibacterium acnes biofilms in acne vulgaris: a case-control study. Br J Dermatol. 2012;167(1):50-58. doi: 10.1111/j.1365-2133.2012.10897.x. PMID: 22356121. Available from: PubMed.
- American Academy of Dermatology Association. Acne: Tips for managing. Last updated November 16, 2022. Accessed July 14, 2026. Available from: AAD.
- Dréno B, Nguyen JM, Hainaut E, et al. Efficacy of Spironolactone Compared with Doxycycline in Moderate Acne in Adult Females: Results of the Multicentre, Controlled, Randomized, Double-blind Prospective and Parallel Female Acne Spironolactone vs doxyCycline Efficacy (FASCE) Study. Acta Derm Venereol. 2024;104:adv26002. doi: 10.2340/actadv.v104.26002. PMID: 38380975. Randomized study in 133 adult women with moderate acne. Both groups used benzoyl peroxide; the doxycycline arm switched to placebo after 3 months while spironolactone continued for 6 months. Available from: PubMed.
- Lai J, Barbieri JS. Acne Relapse and Isotretinoin Retrial in Patients With Acne. JAMA Dermatol. 2025;161(4):367-374. doi: 10.1001/jamadermatol.2024.5416. PMID: 39813053. US MarketScan commercial-claims cohort covering isotretinoin courses completed from 2017 to 2020, with at least 1 year of continuous post-treatment enrollment. Available from: PubMed.
- American Academy of Dermatology Association. Acne: Diagnosis and treatment. Accessed July 14, 2026. Available from: AAD.
- American Academy of Dermatology Association. Are your hair care products causing breakouts? Accessed July 14, 2026. Available from: AAD.
- American Academy of Dermatology Association. Is sports equipment causing your acne? Accessed July 14, 2026. Available from: AAD.
- American Academy of Dermatology Association. Stubborn acne? Hormonal therapy may help. Accessed July 14, 2026. Available from: AAD.
- American Academy of Dermatology Association. Hidradenitis suppurativa: Overview. Accessed July 14, 2026. Available from: AAD.
Medical disclaimer: This article is educational and is not a diagnosis or treatment plan. See a qualified healthcare professional for persistent, painful, scarring, sudden, or severe acne, or before using acne medication during pregnancy or when planning pregnancy.
Stay curious,
Filip