
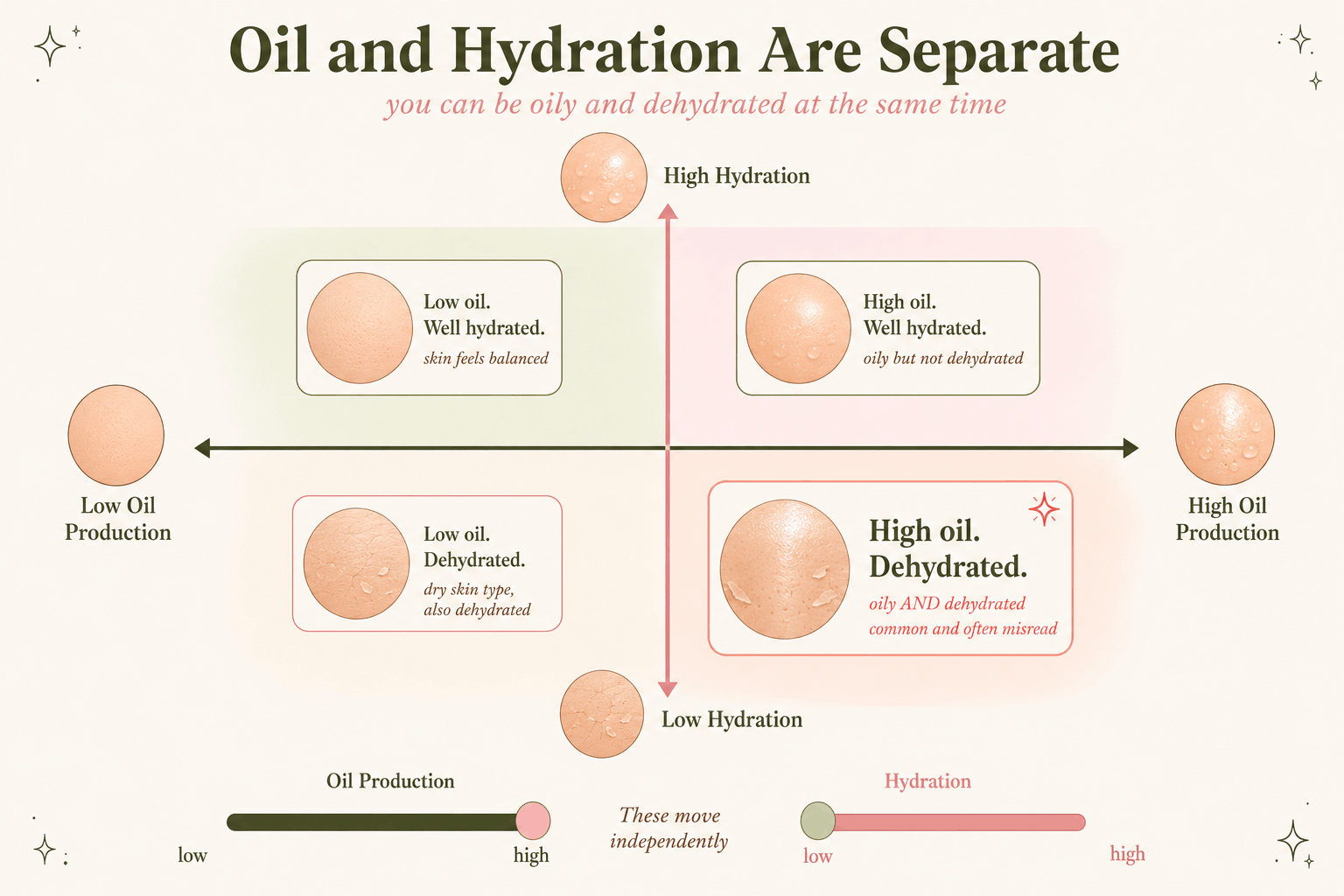
Your skin can be shiny by lunch and still feel tight ten minutes after cleansing. That is not a contradiction. Sebum is oil; hydration is water in the outer layer of the skin. You can have plenty of one and not enough of the other.
The pattern is familiar: an oily T-zone, cheeks that feel tight after washing, foundation clinging to flakes, or a moisturizer that suddenly stings. In that situation, stripping away more oil is usually the wrong instinct. The better question is whether your routine is irritating a skin barrier that was oily to begin with.
“Oily but dehydrated” is not a medical diagnosis. It is a useful description for skin that looks oily but also feels tight, rough, flaky, or unusually sensitive. Start simple: a gentle cleanser, one lightweight moisturizer with a proven humectant such as glycerin, broad-spectrum SPF 30+, and only the acne treatments you actually need. One thing worth dropping is the popular idea that dehydrated skin automatically pumps out extra oil to compensate. That claim is repeated far more often than it is proven.
Table of Contents
What oily but dehydrated skin means
Sebum is the oily material made by sebaceous glands. It lubricates the skin surface, and how much you produce is shaped by things such as genetics, hormones, age, and body area.[1]
Hydration is a separate issue. It refers largely to water in the stratum corneum, the skin’s outermost layer. Barrier function is related, but not identical: when that barrier is disrupted, water escapes more easily and skin can start to feel tight, rough, or sensitive.[2][19]
Think of “oily but dehydrated” as shorthand, not a diagnosis. Persistent redness, itching, greasy scale, burning, painful acne, or repeated reactions to products can point to something else and deserve a closer look.
Why it happens
1. Oily skin plus barrier stress
The most straightforward explanation is often this: your skin naturally runs oily or acne-prone, while your routine or environment is making the surface more irritated and less comfortable. You do not need a dramatic “damaged barrier” story for that to happen.
2. Cleansing too aggressively
Cleansers are not all equally mild. Surfactants, pH, the rest of the formula, contact time, and how often you wash all matter. And no, your face does not need to feel squeaky after cleansing. If it feels tight every time, that is a useful clue that your routine may be too aggressive.[3]
3. Too many active ingredients
Retinoids, benzoyl peroxide, salicylic acid, and azelaic acid can all earn a place in an acne routine. The problem is not that they are “harsh” by definition. The problem is starting several at once, using them too often, and then treating the resulting irritation with even more products.[11]
4. Cold or dry weather
Cold weather and low humidity can make already-dry or dermatitis-prone skin less comfortable. Even an oily face can notice the difference when the air gets drier.[4]
The goal is not to make oily skin dry. The goal is to control oil and acne without wrecking the barrier.
Less stripping, more strategy.Signs and look-alikes
There is no bathroom-mirror test that officially diagnoses “oily but dehydrated skin.” What people usually mean is a combination like this:
- Shine or oil buildup, especially on the forehead, nose, or chin.
- Tightness after cleansing.
- Fine flaking under an oily surface.
- Stinging from products that used to feel normal.
- Makeup separating in oily areas but catching on dry patches.
One warning: not every oily, flaky face is simply “dehydrated.” Acne, rosacea, seborrheic dermatitis, irritant contact dermatitis, and allergic contact dermatitis can overlap with some of these symptoms. When allergic contact dermatitis is suspected, patch testing is the clinical reference standard.[13]
| Pattern | Common clues | What to do |
|---|---|---|
| Acne | Blackheads, whiteheads, pimples, deeper bumps | Use acne treatment, not just moisturizer.[17] |
| Rosacea | Flushing, burning, visible vessels, central redness | Get diagnosis-specific care; rosacea treatment differs from a simple dehydration routine.[14] |
| Seborrheic dermatitis | Greasy scale around brows, nose, scalp, ears | May need antifungal or anti-inflammatory treatment.[15] |
| Contact dermatitis | Itch, burning, rash after product exposure | Stop the suspected trigger. Patch testing may be needed if allergy is suspected. |
Ingredients that help
Glycerin
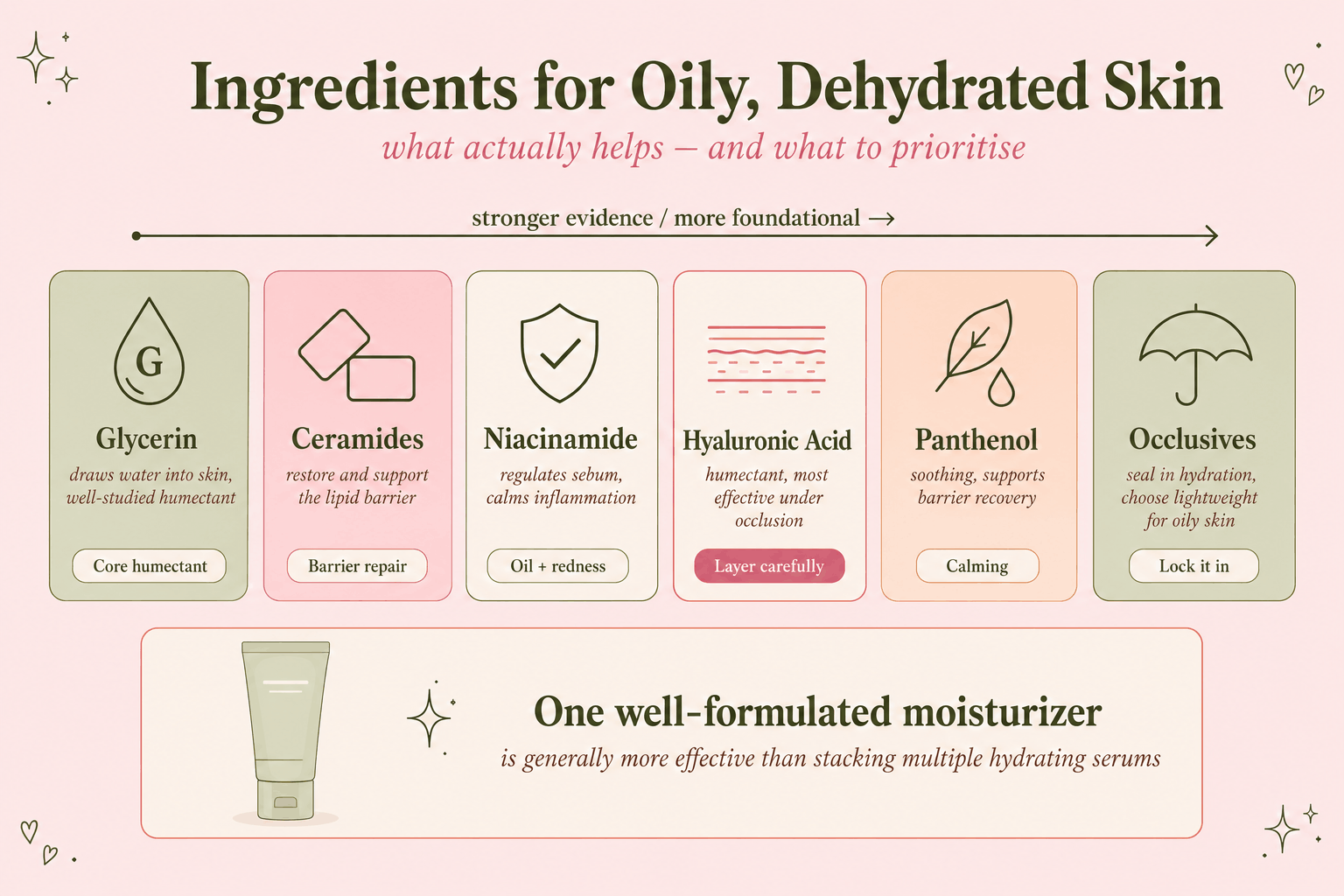
Glycerin is the ingredient I would look for first. It helps the outer skin layer hold on to water, it is common in well-formulated moisturizers, and it has substantial skin-barrier research behind it.[5]
A very sensible first choice Glycerin is inexpensive, widely used, and effective. For most people, a good glycerin-containing moisturizer is more useful than collecting three separate “hydrating” serums.
Ceramides
Ceramides are naturally part of the skin barrier, so including them in a moisturizer can make sense, particularly when acne treatment is drying you out. Just do not shop by ingredient badge alone. A mediocre formula does not become brilliant because “ceramides” appears on the front.[6]
There is also controlled research on a specific ceramide-containing cleanser-and-moisturizer regimen used alongside adapalene/benzoyl peroxide. That regimen improved several signs and measurements of irritation and barrier function. Useful result, yes. Proof that every ceramide cream works the same way, no.[7]
Niacinamide
Niacinamide has a reasonable barrier story behind it. In one paper, nicotinamide increased ceramide and other lipid synthesis in cultured human keratinocytes, and the human part of the work also reported improvements in barrier-related measurements. That is a good reason to consider niacinamide, not a reason to assume every 10% serum will transform your skin.[8]
What about oil control? An older four-week study of a moisturizer with 2% niacinamide found reductions in some facial-sebum measurements, but the results were not identical across cohorts or measurement methods. I would treat oil reduction as a possible bonus, not the main reason to buy it.[9]
Useful, not mandatory Niacinamide can fit well here, but 10% is not a requirement. If your skin already stings easily, a lower-strength formula may be the better buy.
Hyaluronic acid
Hyaluronic acid can improve hydration and make skin feel better, but it is not a magical “barrier repair” switch. Molecular weight, concentration, delivery, and the rest of the formula all influence what you actually get from it.[10]
Panthenol and occlusives
Dexpanthenol is another useful supporting ingredient. It has established moisturizing and barrier-supportive uses in dermatology and is generally well tolerated. Helpful? Yes. A universal cure for every irritated barrier? No.[18]
Occlusives slow water loss from the skin surface. Petrolatum is particularly effective; dimethicone can give a more cosmetically elegant, less greasy feel depending on the formula. Acne-prone skin does not have to avoid petrolatum on principle, but a thick full-face layer is obviously not going to feel good on everyone.
Simple routine
- Cleanse if you need to. Woke up greasy or sweaty? Use a gentle cleanser. Skin feels comfortable? A water rinse may be enough.
- Use a moisturizer you will actually wear. A light lotion or gel-cream with glycerin and emollients is a good place to start.
- Use sunscreen. Choose broad-spectrum SPF 30 or higher. If you need water resistance, check the label for 40- or 80-minute water resistance.[16]
- Take off sunscreen and makeup without turning cleansing into a ritual. Double cleansing is useful when one gentle cleanse does not remove water-resistant sunscreen, makeup, or heavy residue. Otherwise, it is optional.
- Treat the problem you actually have. Use acne treatment for acne, not simply because your face gets shiny.
- Moisturize. Use enough to stop the tight feeling. You do not need to force yourself into a thick cream you hate.
When everything burns
When even bland products start to sting, stop trying to “fix” the situation with another active. Pause scrubs, exfoliating toners, masks, fragrance-heavy products, and anything else you do not actually need. Keep the routine boring for a while: gentle cleanser, moisturizer, sunscreen. If one sunscreen burns, switch formulas and lean on shade, clothing, and a hat while your skin settles. Severe or persistent burning is a medical issue, not a skincare challenge.
What to do if you also have acne
Moisturizer can make acne treatment easier to tolerate, but it is not acne treatment by itself. The 2024 American Academy of Dermatology guideline strongly recommends benzoyl peroxide, topical retinoids, appropriate topical-antibiotic combinations, and oral doxycycline. Salicylic acid, azelaic acid, clascoterone, minocycline, sarecycline, combined oral contraceptives, and spironolactone receive conditional recommendations. Isotretinoin is recommended for severe, scarring, or treatment-resistant acne.[11][12]
| Treatment | Evidence position | Barrier note |
|---|---|---|
| Topical retinoid | Strong AAD recommendation | Early dryness is common. Prescription directions often say once daily, but clinicians may adjust the introduction when irritation is hurting adherence. |
| Benzoyl peroxide | Strong AAD recommendation | Effective for inflammatory acne. It is also paired with topical antibiotics to help reduce the risk of bacterial resistance. |
| Salicylic acid | Conditional AAD recommendation | Useful for clogged pores, but avoid stacking several salicylic products at once. |
| Azelaic acid | Conditional AAD recommendation for acne | Can help acne and post-acne discoloration, but may sting on irritated skin. |
- Add only one irritating active at a time.
- Follow the label or clinician instructions.
- For many facial retinoids, a thin pea-sized amount is commonly used for the entire face.
- Burning and heavy peeling are not proof that a product is working.
- Get help for nodules, scarring, severe inflammation, or acne that is not improving.
What to look for in products
| Product | Look for | Avoid when reactive |
|---|---|---|
| Cleanser | Gentle, non-scrubby, rinses without tightness | Harsh scrubs, strong fragrance, “squeaky clean” feel |
| Moisturizer | Glycerin, light emollients, maybe ceramides | Buying too many serums instead of one complete formula |
| Sunscreen | Broad-spectrum SPF 30+, comfortable texture | Formulas that sting badly or pill so much you underapply |
| Acne active | One evidence-based active used consistently | Layering retinoid, acid, benzoyl peroxide, and scrub together |
Myths to ignore
| Claim | Better answer |
|---|---|
| “Dehydrated skin makes extra oil to compensate.” | The evidence is not strong enough to state this as a rule. An aggressive routine can irritate your skin while you remain oily. |
| “Oily skin does not need moisturizer.” | You can have plenty of sebum and still benefit from a moisturizer. Oil production and barrier hydration are not the same measurement. |
| “If an acid burns, it is working.” | No. Burning tells you the product is irritating your skin. It does not tell you the treatment is more effective. |
| “Hyaluronic acid fixes the skin barrier.” | It can help with hydration. Repairing and supporting the barrier depends on the complete formula, not one fashionable ingredient. |
| “Mineral sunscreen is always irritation-free.” | Mineral filters are often suggested when sunscreen stings or for conditions such as rosacea, but a finished sunscreen can still be uncomfortable for an individual user. |
What the evidence actually supports
Strip away the marketing language and the useful core is fairly simple: cleanse without leaving your skin tight, use a complete moisturizer, wear sunscreen, and treat acne with treatments that actually target acne.
Oil production and water content are not the same thing. Gentle cleansing, moisturization, and evidence-based acne treatment all have a solid place here.
You do not need a seven-step hydration routine. One well-formulated moisturizer can do most of the heavy lifting.
The routine usually falls apart when people keep adding acids, scrubs, masks, and strong actives to skin that is already irritated.
Persistent redness, greasy scale, itching, burning, or painful bumps may be a skin condition that needs an actual diagnosis.
The useful takeaway is simple. Oily skin is not the enemy, and the goal is not to dry it into submission. Control acne or excess oil where needed, but keep the barrier comfortable enough that you can stay consistent.
Frequently asked questions
Can skin really be oily and dehydrated?
Yes. Sebum and water in the outer skin layer are separate variables. A shiny face can still feel tight, rough, or flaky.
Does dehydration make skin produce more oil?
Not as a reliable rule. Harsh cleansing can leave skin irritated and tight while it remains oily, but that is not the same as proving a compensatory surge in sebum.
What moisturizer should I use?
Start with a lightweight lotion or gel-cream containing glycerin plus emollients. Ceramides can be useful, but the complete formula matters more than one word on the label.
Is hyaluronic acid enough?
Usually not by itself. Hyaluronic acid can help hydration, but a complete moisturizer is often more useful than relying on a watery serum alone.
Should I stop retinoids or salicylic acid?
No, not automatically. They may be treating real acne. Cut unnecessary overlap and adjust use when irritation starts becoming the bigger problem.
How long does barrier recovery take?
There is no universal countdown. Mild irritation may settle fairly quickly after the trigger is removed; dermatitis can last longer and may need treatment.
Can I use petrolatum?
Yes, if you tolerate it. On oily skin, a small amount on irritated patches may feel far better than coating the whole face.
When should I see a dermatologist?
Book an assessment for severe burning, persistent itching, greasy scale, flushing, painful acne, scarring, or symptoms that do not improve after simplifying your routine.
References
- Shamloul G, Khachemoune A. An updated review of the sebaceous gland and its role in health and diseases Part 1: Embryology, evolution, structure, and function of sebaceous glands. Dermatol Ther. 2021 Jan;34(1):e14695. doi: 10.1111/dth.14695. Epub 2021 Jan 1. PMID: 33354858. Available from: PubMed.
- Berardesca E, Loden M, Serup J, Masson P, Rodrigues LM. The revised EEMCO guidance for the in vivo measurement of water in the skin. Skin Res Technol. 2018 Aug;24(3):351-358. doi: 10.1111/srt.12599. Epub 2018 Jun 20. PMID: 29923639. Available from: PubMed.
- Ananthapadmanabhan KP, Moore DJ, Subramanyan K, Misra M, Meyer F. Cleansing without compromise: the impact of cleansers on the skin barrier and the technology of mild cleansing. Dermatol Ther. 2004;17 Suppl 1:16-25. doi: 10.1111/j.1396-0296.2004.04s1002.x. PMID: 14728695. Available from: PubMed.
- Engebretsen KA, Johansen JD, Kezic S, Linneberg A, Thyssen JP. The effect of environmental humidity and temperature on skin barrier function and dermatitis. J Eur Acad Dermatol Venereol. 2016 Feb;30(2):223-49. doi: 10.1111/jdv.13301. Epub 2015 Oct 8. PMID: 26449379. Available from: PubMed.
- Fluhr JW, Darlenski R, Surber C. Glycerol and the skin: holistic approach to its origin and functions. Br J Dermatol. 2008 Jul;159(1):23-34. doi: 10.1111/j.1365-2133.2008.08643.x. Epub 2008 Jul 1. PMID: 18510666. Available from: PubMed.
- Schild J, Kalvodová A, Zbytovská J, Farwick M, Pyko C. The role of ceramides in skin barrier function and the importance of their correct formulation for skincare applications. Int J Cosmet Sci. 2024 Aug;46(4):526-543. doi: 10.1111/ics.12972. PMID: 39113291. Available from: PubMed.
- Draelos ZD, Baalbaki N, Colon G, Dreno B. Ceramide-Containing Adjunctive Skin Care for Skin Barrier Restoration During Acne Vulgaris Treatment. J Drugs Dermatol. 2023 Jun 1;22(6):554-558. doi: 10.36849/JDD.7142. PMID: 37276158. Available from: PubMed.
- Tanno O, Ota Y, Kitamura N, Katsube T, Inoue S. Nicotinamide increases biosynthesis of ceramides as well as other stratum corneum lipids to improve the epidermal permeability barrier. Br J Dermatol. 2000 Sep;143(3):524-31. doi: 10.1111/j.1365-2133.2000.03705.x. PMID: 10971324. Available from: PubMed.
- Draelos ZD, Matsubara A, Smiles K. The effect of 2% niacinamide on facial sebum production. J Cosmet Laser Ther. 2006 Jun;8(2):96-101. doi: 10.1080/14764170600717704. PMID: 16766489. Available from: PubMed.
- Bravo B, Correia P, Gonçalves Junior JE, Sant'Anna B, Kerob D. Benefits of topical hyaluronic acid for skin quality and signs of skin aging: From literature review to clinical evidence. Dermatol Ther. 2022 Dec;35(12):e15903. doi: 10.1111/dth.15903. Epub 2022 Oct 21. PMID: 36200921; PMCID: PMC10078143. Available from: PubMed.
- Reynolds RV, Yeung H, Cheng CE, Cook-Bolden F, Desai SR, Druby KM, Freeman EE, Keri JE, Stein Gold LF, Tan JKL, Tollefson MM, Weiss JS, Wu PA, Zaenglein AL, Han JM, Barbieri JS. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024 May;90(5):1006.e1-1006.e30. doi: 10.1016/j.jaad.2023.12.017. Epub 2024 Jan 30. Erratum in: J Am Acad Dermatol. 2026 Jul;95(1):347. doi: 10.1016/j.jaad.2026.04.009. PMID: 38300170. Available from: PubMed.
- American Academy of Dermatology. American Academy of Dermatology issues updated guidelines for the management of acne. Published January 31, 2024. Accessed July 11, 2026. Available from: American Academy of Dermatology.
- Johansen JD, Aalto-Korte K, Agner T, Andersen KE, Bircher A, Bruze M, Cannavó A, Giménez-Arnau A, Gonçalo M, Goossens A, John SM, Lidén C, Lindberg M, Mahler V, Matura M, Rustemeyer T, Serup J, Spiewak R, Thyssen JP, Vigan M, White IR, Wilkinson M, Uter W. European Society of Contact Dermatitis guideline for diagnostic patch testing - recommendations on best practice. Contact Dermatitis. 2015 Oct;73(4):195-221. doi: 10.1111/cod.12432. Epub 2015 Jul 14. PMID: 26179009. Available from: PubMed.
- van Zuuren EJ, van der Linden MMD, Arents BWM. Rosacea treatment guideline for the Netherlands. Br J Dermatol. 2020 Jun;182(6):1504-1506. doi: 10.1111/bjd.18882. Epub 2020 Feb 20. PMID: 31970753; PMCID: PMC7317907. Available from: PubMed Central.
- American Academy of Dermatology. Seborrheic dermatitis: Diagnosis and treatment. Updated May 14, 2024. Accessed July 11, 2026. Available from: American Academy of Dermatology.
- American Academy of Dermatology. How to select a sunscreen. Accessed July 11, 2026. Available from: American Academy of Dermatology.
- Oge' LK, Broussard A, Marshall MD. Acne Vulgaris: Diagnosis and Treatment. Am Fam Physician. 2019 Oct 15;100(8):475-484. PMID: 31613567. Available from: PubMed.
- Ebner F, Heller A, Rippke F, Tausch I. Topical use of dexpanthenol in skin disorders. Am J Clin Dermatol. 2002;3(6):427-33. doi: 10.2165/00128071-200203060-00005. PMID: 12113650. Available from: PubMed.
- Rogiers V; EEMCO Group. EEMCO guidance for the assessment of transepidermal water loss in cosmetic sciences. Skin Pharmacol Appl Skin Physiol. 2001 Mar-Apr;14(2):117-28. doi: 10.1159/000056341. PMID: 11316970. Available from: PubMed.
Medical disclaimer: This article is for education only and is not medical advice. Persistent redness, severe itch, painful acne, scarring, swelling, crusting, or recurring reactions should be assessed by a qualified healthcare professional.
Hot girls read the research.